

Journal of the Bahrain Medical Society
Year 2018, Volume 30, Issue 3, Pages 34-41
https://doi.org/10.26715/jbms.3_28122018Arif Maldar*1, Suhas M1
1Department of General Medicine, Jawaharlal Nehru Medical College, KLES University, Nehru Nagar, Belagavi 590010, Karnataka, India.
*Corresponding author:
Arif Maldar, Department of General Medicine, Jawaharlal Nehru Medical College, KLES University, Nehru Nagar, Belagavi 590010, Karnataka, India; Tel: (+91) 9343227719, Email: arifmaldar@yahoo.com
Received date: December 6, 2018; Accepted date: December 28, 2018; Published date: December 31, 2018

Background and objectives: Among several non invasive techniques available, a high-resolution B-mode ultrasonography is the widely used technique to measure carotid intima-media thickness (CIMT) in rheumatoid arthritis (RA) patients with elevated cardiovascular risk. The present study was undertaken to explore the clinical relationship between CIMT and disease activity in patients with RA.
Methods: This study involved 50 adult patients with RA. Demographic, physical, systemic, and clinical data and history of the patients were recorded. Investigations, such as erythrocyte sedimentation rate, highly sensitive C-reactive protein, renal and liver function tests, RA factor, and anticyclic citrullinated peptide antibody tests were performed. CIMT was assessed using high resolution B-mode ultrasonography and the disease severity was assessed based on disease activity score (DAS) 28.
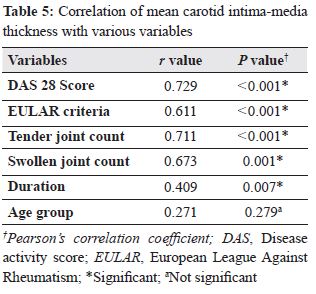
Results: The mean age of the RA patients was 49.88 ± 12.12 years with male predilection. The mean duration, mean European League Against Rheumatism (EULAR) criteria score, and mean DAS 28 score in RA patients were 3.62 ± 3.25 years, 8.10 ± 1.58, and 4.91 ± 1.11, respectively. The mean CIMT observed in RA patients was 0.94 ± 0.31 cm. Significant difference was observed in the mean CIMT values of different variables, including duration of joint pain (P = 0.007), tender joint count(P < 0.001), swollen joint count (P < 0.001), EULAR criteria score (P < 0.001), and DAS 28 score(P < 0.001). Also, CIMT correlated positively with tender joint count (r = 0.711; P < 0.001), swollen joint count (r = 0.673; P < 0.001), EULAR criteria score (r = 0.611; P < 0.001), and DAS 28 score (r = 0.729; P < 0.001).
Conclusion: A strong correlation was observed between CIMT and disease activity in patients with RA. Hence, CIMT can be a useful surrogate marker for detecting atherosclerosis in patients with RA.
Keywords: Atherosclerosis, carotid artery intima-media thickness, European League Against Rheumatism, High-resolution B-mode ultrasonography, rheumatoid arthritis
Rheumatoid arthritis (RA), a chronic inflammatory disease, affects 0.5–1% of the population with life expectancy shortened by 3–18 years.1, 2 Cardiovascular disease is considered as the leading cause of morbidity and mortality in patients with RA.2 Traditional risk factors, including age, gender, smoking, diabetes, hypercholesterolemia, hypertension, sedentary lifestyle, and family history of early coronary artery disease have been attributed in the pathophysiology of atherosclerosis.3 However, the relationship between traditional risk factors and atherosclerosis in RA patients is still unclear.4
In addition to traditional risk factors, RA-specific risk factors, such as disease activity, inflammatory markers and anti-cyclic citrullinated peptide (CCP) have been associated with cardiovascular risk and increased carotid intima-media thickness (CIMT).5 Among these, the inflammatory pathway that damages the bone, cartilage, soft tissue, viscera, and blood vessels has been implicated as a pathogenetic risk factor in the pathobiology of atherosclerosis.6, 7 At present, many noninvasive screening techniques have been emerged to assess the association between surrogate markers and development of atherosclerosis in RA patients. One among those is evaluation of CIMT by high-resolution B-mode ultrasonography. Hence, it is the independent risk factor to evaluate prognosis of cardiovascular diseases. It is a simple, economical, reliable, noninvasive index being increasingly used in the detection of subclinical atherosclerosis.2 In addition, CIMT has been employed as an ideal surrogate endpoint marker in several clinical trials to assess the progression or regression of atherosclerosis.8
Ethnic group, such as Asian Indians are more prone to high-risk of metabolic syndrome and premature atherosclerosis.9 Therefore, Indian patients with RA are at an augmented risk of developing atherosclerosis. However, South Indian data about the burden of atherosclerosis among patients with RA is scarce. Hence, this study was undertaken to explore the correlation between disease activity of RA and CIMT, a surrogate marker of atherosclerosis, to identify high-risk RA patients who may benefit from active therapy to overcome this condition.
The present cross-sectional study was conducted for 1 year (January–December 2014) at the department of Medicine. Ethical approval was obtained from Institutional Ethical and Research Committee. Sample size calculation of the study was based on 80% of average hospital statistics on patients with RA for the last 3 years. Out of 53 patients attended, 50 patients fulfilled the selection criteria. Patients screened based on selection criteria were informed about the nature of the study and enrolled after obtaining a written informed consent.
Inclusion criteria were patients aged 18–80 years diagnosed with RA based on the history, clinical examination, and the American College of Rheumatology (ACR) approved and the European League Against Rheumatism (EULAR) criteria.10 In addition, the patients willing to undergo carotid artery imaging to measure CIMT using high resolution B-mode ultrasonography were included in the study. Patients with a history suggestive of type II diabetes mellitus, hypertension, cerebrovascular disease, peripheral vascular disease, coronary artery disease, chronic hepatic failure, hypothyroidism, and chronic renal failure were excluded from the study. Patients with pregnancy or history of pregnancy (within 3 months) were also exempted from the study.
Sociodemographic data and personal, medical, and treatment history of all the patients were recorded. A thorough physical examination was conducted for vitals (blood pressure, pulse rate, and respiratory rate) followed by a systemic examination. During the clinical examination the number of swollen joints and tender joints were observed and recorded. These findings were noted on a predesigned and pretested proforma.
Venous blood (10 mL) was collected from the median cubital vein and assessed for erythrocyte sedimentation rate (ESR), highly sensitive C-reactive protein, renal and liver function tests, RA factor, anti-CCP antibody, and high-resolution B-mode ultrasonography mode to measure the CIMT. Anti-CCP antibody test was done using ELISA (Enzyme-linked immune sorbent assay) method.11 Patients with anti-CCP titers more than 10 IU/dL were considered as positive. The severity of the disease was calculated using Disease Activity Score (DAS) 28.12
Ultrasonic evaluation of the carotid arteries was done using PHILIPS HD-11 equipped with a 7.5 MHz linear array transducer. The maximum IMT was measured at the internal, near as well as far walls of the common carotid artery, and the bifurcation; was expressed as mean aggregate value. The IMT was evaluated as normal if it didn’t exceed 1 mm. All scans were conducted by an experienced sonographer, without prior knowledge about clinical as well as angiographic characteristics of the patients.
SPSS 20 was used to analyze the data. The categorical data were expressed in terms of rates, ratios, and percentages. Chi square or Fisher's exact test were used to determine the differences in categorical characteristics. Continuous data were compared using independent sample t-test. In case of more than two means, the comparison was done using one-way ANOVA. The correlation between CIMT and disease severity was determined using Pearson’s correlation coefficient. P ≤ 0.050 at 95% confidence interval was considered statistically significant.
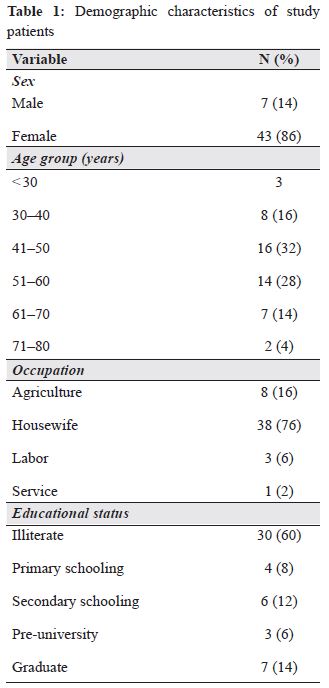
The demographics, including disease-related variables in patients with RA are summarized in Tables 1 and 2. Most of the patients in this study were aged between 41 and 60 years with a mean age of 49.88 ± 12.12 years. The mean duration of joint pain and RA were 45 ± 2.16 years and 3.62 ± 3.25 years, respectively. The mean EULAR criteria score, mean ESR value, and mean DAS 28 score noted in the patients were 8.10 ± 1.58, 50.68 ± 24.73 mm/h, and 4.91 ± 1.11, respectively.
*Table 2, 3 and 4 are in PDF
The hematological, renal, and liver profile of study patients is given in Table 3. The mean CIMT in RA patients was 0.94 ± 0.31 cm. Whereas, median CIMT was 0.90 cm with minimum and maximum being 0.50 cm and 1.85 cm, respectively. The comparison of mean CIMT with disease variables is shown in Table 4. A significant rise in CIMT was observed with respect to disease activity based on DAS 28 score, increased EULAR criteria score, swollen joint counts, tender joint counts, and duration of disease (P < 0.001). While, mean CIMT levels increased, with respect to RA factor, anti-CCP antibodies, age, and gender, were not statistically significant (P > 0.005).
The comparison of mean CIMT with disease variables is shown in Table 5. A strong correlation was observed between mean CIMT and DAS 28 score, EULAR criteria score, swollen joint count, tender joint count, and duration. However, a weak correlation was observed between mean CIMT and age group in patients.
A striking similarity was observed between inflammatory pathway in atherosclerosis and RA. However, instead of eliminating systemic inflammation and focusing on treating the patients with joint manifestations may cause adverse effects in patients with RA.3 However, to date very few studies13 have evaluated the relationship of disease activity in RA patients with CIMT in south India. Hence, this study was designed to evaluate the clinical relationship between CIMT and disease activity in RA patients.
Women are affected three times more by RA than men; however, sex differences diminish in the older age group.13, 14 Similarly, in our study, women outnumbered men. Other studies in the literature exhibit a similar sex distribution.13, 16 Literature revealed that individuals aged between 35 and 50 years are more prone to RA and its prevalence increases with age till 70 years and then declines, which is comparable with our study.17 Raised ESR levels in this study demonstrated that most of the patients had severe disease activity. However, this cannot be used solely for diagnosing RA. It is very helpful in the diagnosis and follow-up of RA patients when used with other diagnostic parameters.18 A study by Sinha et al. reported that RA is more severe in patients with positive RA factor,19 which is observed similarly in our study. In contrast, a meta-analysis conducted by Kawano et al.20 reported that anti-CCP antibodies are more sensitive and specific than RA factor in diagnosing RA patients.
The mean CIMT observed in this study was similar to that of a case-control study by Sing et al.13 in which the mean CIMT in RA group was 0.80 ± 0.15 mm. Similarly, a case-control study by Balaraju et al.21 observed a positive correlation between inflammation (severity and duration) and intima-media thickness and recorded mean CIMT as 0.798 ± 0.19 mm in RA patients. Further, there was a two-fold increase in mean CIMT in patients with severe disease activity compared to mild ones. Moreover, a similar trend of mean CIMT values and the correlation was noticed with DAS 28 score, EULAR criteria score, swollen wrist count, and swollen joint count. The head to head comparison of findings observed in this study was not possible due to lack of similar studies in the literature. Despite the methodological differences and variation in sample size, the finding of the present study corroborates with the studies in the literature.9, 21 Overall, these findings indicate higher CIMT in patients with RA and a positive association as well as correlation of CIMT with disease severity.
Disease duration is one of the best predictors for the development of atherosclerotic disease. Moreover, the CIMT increases significantly with duration of disease. Studies conducted also observed a statistically significant association of disease duration with CIMT and atherosclerotic plaques.2, 13 This may be due to increased inflammation and other factors, such as increased arterial stiffness22 and prothrombotic marker in RA patients.23 Likewise, in our study, significantly higher CIMT values and symptoms of subclinical atherosclerosis were noticed in patients with longer disease duration. A study by Dengel et al.24 reported that the mean intimal thickness observed in men with RA was significantly greater than that in women with RA (0.420 ± 0.004 mm vs. 0.444 ± 0.004 mm, P = 0.01). This indicates that vascular involvement in men with RA is more severe than in women with RA. However, in our study, the mean CIMT values in men and women were comparable. Further, the mean CIMT values in RA patients in this study were not statistically different with respect to RA factor, anti-CCP antibodies, and age group. In contrast to literature, CIMT was less in RA positive patients compared to RA negative patients. Similarly, a study conducted by Dessein et al. reported that CIMT was not influenced by RA status.25 In contrast, a study by Merza et al.26 revealed that patients with seropositive RA factor had statistically higher mean CIMT values than seronegative patients (0.72 ± 0.10 mm vs. 0.57 ± 0.08 mm; P < 0.001). Furthermore, a significant relationship was observed between age and mean CIMT values, which might be due to the disease course and chronic inflammatory processes. Also, in contrast, a study conducted by van Zeben et al.5 observed a statistically positive correlation between anti-CCP positivity and CIMT, though it was not significant (P = 0.078).
The study has few limitations. Firstly, a threshold for demarcating normal and abnormal values of CIMT as a marker for atherosclerosis was not clear. Hence, this limited the study to explore the association of several aspects, such as age, gender, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP). Also, the methods available for defining the cut-off value do not appear to be ideal, hence, were not considered in this study. Secondly, as this study design was a cross-sectional study it limits the study from observing for clinical events, which reflects the consequences of atherosclerosis in long-term.
Overall, CIMT serves as a useful surrogate marker for detecting atherosclerosis in patients with RA. Based on the findings, the current study lights a strong relationship of CIMT not only with the disease per se, but also with the disease severity as determined by DAS 28 score, which considers various characteristics, such as swollen joint and tender joint counts, EULAR criteria score, and duration of disease. Furthermore, this study is a single-center study with a limited sample size, therefore, the results obtained couldn’t be generalized to the whole RA patients. Therefore, studies with larger sample size are required to validate these findings.
The authors of the study have no conflict of interest to declare.
Both the authors have contributed equally in the development of the manuscript.
1. McInnes IB, Schett G. The pathogenesis of rheumatoid arthritis. N Engl J Med. 2011;365:2205-19.
2. Targonska-Stepniak B, Drelich-Zbroja A, Majdan M. The relationship between carotid intima-media thickness and the activity of rheumatoid arthritis. J Clin Rheumatol. 2011;17:249-55.
3. Ku IA, Imboden JB, Hsue PY, et al. Rheumatoid arthritis. Circulation. 2009;73:977-85.
4. Myasoedova E, Gabriel SE. Cardiovascular disease in rheumatoid arthritis: A step forward. Curr Opin Rheumatol. 2010;22:342-7.
5. van Zeben D, Klop B, van de Geijn G-JM, et al. Association of cardiovascular risk factors with carotid intima media thickness in patients with rheumatoid arthritis with low disease activity compared to controls: a cross-sectional study. PLoS One. 2015;10:e0140844.
6. Gonzalez-Gay MA, Gonzalez-Juanatey C, Martin J, editors. Rheumatoid arthritis: A disease associated with accelerated atherogenesis. Semin Arthritis Rheum. 2005;35:8-17.
7. Mahajan V, Handa R, Kumar U, et al. Assessment of atherosclerosis by carotid intimomedial thickness in patients with rheumatoid arthritis. J Assoc Physicians India. 2008;56:587-90.
8. Patel S, Bhatt K, Patel A, et al. A study of carotid intimomedial thickness as a primary marker of atherosclerosis in patients with rheumatoid arthritis. ICF Journal. 2017;9:31-5.
9. Mohan A, Sada S, Kumar BS, et al. Subclinical atherosclerosis in patients with rheumatoid arthritis by utilizing carotid intima-media thickness as a surrogate marker. Indian J Med Res. 2014;140:379-86.
10. Entezami P, Fox DA, Clapham PJ, et al. Historical perspective on the etiology of rheumatoid arthritis. Hand Clin. 2011;27:1-10.
11. Suzuki K, Sawada T, Murakami A, et al. High diagnostic performance of ELISA detection of antibodies to citrullinated antigens in rheumatoid arthritis. Scand J Rheumatol. 2003;32:197-204
12. Fransen J, Stucki G, van Riel PL. Rheumatoid arthritis measures: Disease Activity Score (DAS), Disease Activity Scoreâ€28 (DAS28), Rapid Assessment of Disease Activity in Rheumatology (RADAR), and Rheumatoid Arthritis Disease Activity Index (RADAI). Arthritis Care Res. 2003;49:S214–S24.
13. Singh H, Goyal M, Sen J, et al. Correlation of intima-media thickness (as a marker of atherosclerosis) with activity and duration of rheumatoid arthritis using carotid ultrasound. J Indian Acad Clin Med. 2011;12:15-20.
14. Ahlmén M, Svensson B, Albertsson K, et al. Influence of gender on assessments of disease activity and function in early rheumatoid arthritis in relation to radiographic joint damage. Ann Rheum Dis. 2010;69:230-3.
15. Areskougâ€Josefsson K, Öberg U. A literature review of the sexual health of women with rheumatoid arthritis. Musculoskeletal Care. 2009;7:219-26.
16. lateef Jassim NA, Saeed BN, Gorial FI. Carotid intima-media thickness in rheumatoid arthritis detected by doppler ultrasound. Al- Kindy Col Med J. 2009;5:54-8.
17. Naidich TP, Castillo M, Cha S. Imaging of the spine. 1st Edition ed. Philadelphia: Elsevier Health Sciences; 2011.p.457.
18. Shankar S, Grover R, Handa R. Role of anticyclic citrullinated peptide antibodies in erosive disease in patients with rheumatoid arthritis. Indian J Med Res. 2006;124:689-96.
19. Sinha RP, Agarwal D, Bansal D. Risk of subclinical atherosclerosis in patients with rheumatoid arthritis in India. Journal of Evolution of Medical and Dental Sciences. 2015;4:13233-9.
20. Kawano S, Saigo K, Morinobu A, et al. Meta-analysis: Diagnostic accuracy of anticyclic citrullinated peptide antibody and rheumatoid factor for rheumatoid arthritis. Ann Intern Med. 2007;146:797-808.
21. Balaraju G, Nagamani R, Sridhar D, et al. Correlation of intima media thickness (as a marker of atherosclerosis) with activity and duration of rheumatoid arthritis using carotid ultrasound. International Journal of Scientific and Research Publications. 2015;5:1-11.
22. del Rincón I, Freeman GL, Haas RW, et al. Relative contribution of cardiovascular risk factors and rheumatoid arthritis clinical manifestations to atherosclerosis. Arthritis Rheum. 2005;52:3413-23.
23. Mameli A, Barcellona D, Marongiu F. Rheumatoid arthritis and thrombosis. Clin Exp Rheumatol. 2009;27:846-55.
24. Dengel DR, Jacobs DR, Steinberger J, et al. Gender differences in vascular function and insulin sensitivity in young adults. Clin Sci. 2011;120:153-60.
25. Dessein PH, Norton GR, Badenhorst M, et al. Rheumatoid arthritis impacts on the independent relationships between circulating adiponectin concentrations and cardiovascular metabolic risk. Mediators of Inflammation. 2013;2013:1-9.
26. Merza RR, Fateh SM, Ehsan HA. Measurement of the common carotid arteries intima-media thickness by ultrasonography in patients with rheumatoid arthritis. Cukurova Med J. 2014;39:213-23.