

Journal of the Bahrain Medical Society
Year 2018, Volume 30, Issue 1, Pages 14-21
https://doi.org/10.26715/jbms.1_02022018Muna Ahmed Awn1*, Nooralhoudh Ali1, Hessa Al Saqer1, Duaa Al Laith1, Adel Al Sayyad1
1Family Practice Residency Program, Ministry of Health - Kingdom of Bahrain. P.O. Box 42.
*Corresponding author:
Muna Ahmed Awn, Family Practice Residency Program, Ministry of Health - Kingdom of Bahrain. P.O. Box 42; Tel: (+973) 17263597, Fax: (+973) 17251104, Email: mona84oun@gmail.com
Received date: June 15, 2017; Accepted date: February 02, 2018; Published date: March 20, 2018

Background and objectives: Primary nocturnal enuresis is the bedwetting tendency in children aged ≥ 5 years, who have not stayed dry during sleep, for a period of more than 6 months. Secondary nocturnal enuresis is the recurrence of bedwetting after continuous a dry period of more than 6–12 months. The primary objective of the study was to estimate the prevalence of nocturnal enuresis (NE) among children aged 5–12 years, who received primary healthcare in Bahrain. The secondary objective was to determine the prevalence of primary and secondary NE, and the factors associated with primary NE.
Methods: This is a cross-sectional analytical study conducted in children aged 5–12 years, who attended local health centers in Bahrain in June 2015. A total of 438 children from eight local health centers were included in the study. A self-administered questionnaire was used as the assessment tool.
Results: The overall prevalence of NE in Bahrain was 11.1%. The prevalence of primary NE and secondary NE was 82% and 18%, respectively. A significant association was established between NE and father’s education (P = 0.003), number of siblings (P = 0.045), and father’s (P = 0.033), mother’s (P < 0.001), and sibling’s (P < 0.001) history of NE.
Conclusion: The prevalence of NE in Bahrain is similar to that observed in other studies. Further studies are required to assess the prevalence of secondary enuresis and its associated factors.
Keywords: Prevalence, enuresis, children, primary care, Bahrain
Enuresis is defined as the involuntary voiding of urine, occurring at least twice a week for 3 months.1 Nocturnal enuresis (NE), also known as bedwetting, is defined as any intermittent incontinence that occurs while a child, at least 5 years old, is asleep.1 NE can be either primary or secondary.
Primary NE is bedwetting in children aged ≥ 5 years, who have never been dry during sleep, for a period of more than 6 months.2 Secondary NE is the onset of bedwetting after a continuous dry period of more than 6–12 months.2 The overall prevalence of NE varies in different countries and amongst different age groups, ranging from 2.3–25%.3 Studies have shown that the prevalence of NE declines with age.4, 5 There are many other factors that are associated with the development of NE such as gender1, education and profession of the mother, income of the family6, family history of NE7, sleep pattern, and large family size.8 Parental divorce or a separated family, social class, and family stress have also been shown to have a significant association with the prevalence of NE.9, 10 Sleep problems are considered to be a significant factor associated with NE.11 Moreover, the prevalence of NE is significantly associated with a history of urinary tract infection.12 Finally, there is also a high prevalence of NE among patients with sickle cell disease, thalassemia major, and constipation.13, 14
When evaluating a child with NE, determining family and medical history is crucial to determine the underlying risk factors or causes, as well as the impact NE has on the child and his/her family. It is also important to detect and treat NE, as early as possible, as it may have a substantial psychosocial impact that leads to behavioral and social problems, effecting the child’s quality of life and school performance as well as a significant risk of emotional and physical abuse.15, 16 The family physician is in a prime position to screen, detect, and treat NE, as early as possible, to prevent these consequences.12
The study was first submitted to the ethical committee in the Ministry of Health for evaluation and was approved. Then a cross-sectional analysis, involving a self-administered questionnaire, was used to determine the prevalence of NE in children in Bahrain aged 5–12 years and associated factors, during the month of June 2015. The necessary study sample size was calculated using an automated sample size calculator online 18 and utilized the population size of 148,371 children in Bahrain aged 5–14 years from the census conducted in 2010.19 The sampling technique used, consisted of multistage sampling. The total number of children was stratified according to the 4 governorates. Fromeach governorate, two health centers were randomly selected. A total of 458 children were chosen from eight local health centers randomly selected from the governorates. The confidence level was 95% (P ≤ 0.05).
For each health center, parents of children aged 5–12 years were selected using convenience sampling. This was achieved by selecting eligible parents at the registration counter.
Criteria for parent inclusion were:
Criteria for parent exclusion were:
Consent was obtained, and language preference was identified. A questionnaire was given to the parent to be filled out and returned when finished. The questionnaire was self-administered in either Arabic or English. The identity of study participants remained anonymous. The questionnaire was designed and divided into four parts as follows:
The questionnaire was revised by medical doctors, specialized in treating NE, for content validation. Proper translation between Arabic and English was ensured. A pilot study was conducted with approximately 30 patients in the BBK Hidd Health Center and East Riffa Health Center to test the proposed methodology of the research project.
The data collected from the questionnaires was entered into the computer, imported into a database, and revised for accuracy. The data was analyzed using Statistical Package for the Social Sciences (SPSS) 22. Frequency and percent distributions were used for all demographic data, prevalence, associated factors, management, and impact variables in the study. Cross tabulation was used between the prevalence of NE and each demographic variable, as well as each associated factor variable. The chi-square and Fisher’s exact
tests were used to determine whether there were significant relationships between the prevalence of NE and the demographic data or associated factor variables. A P value of < 0.05 was considered statistically significant.
A total of 458 questionnaires were distributed among patients of the eight selected local health centers. Two patients were nonresponders. Of the 456 questionnaires returned by the patients, 438 were considered eligible for inclusion in the study.
The study was conducted among children aged 5–12 years old. Table 1 demonstrates the demographic characteristics of children, who were patients of primary healthcare in Bahrain, and their parents.
Table 1: Demographic characteristics of children who were patients of primary healthcare, and their parents.
 *The difference between the sample size (n = 438) and the total sample size mentioned in the table is due to missing data.
*The difference between the sample size (n = 438) and the total sample size mentioned in the table is due to missing data.
Frequencies of health behavioral conditions of children who are patients of primary healthcare in Bahrain and percent distribution of associated factors are shown in Table 2.
Table 2: Frequency of health and behavioral conditions of children who were patients of primary healthcare in Bahrain, and percent distribution of associated factors.
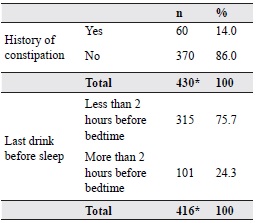
*The difference between the sample size (n = 438) and the total sample size mentioned in the table is due to missing data.
Out of the 438 children participating in the study, 47 children were found to meet the criteria for the diagnosis of NE. Questions regarding the prevalence of NE were only completely answered by 425 patients, meaning 13 responses were missing. Based on the obtained data, the overall prevalence of NE was 11.1% among all age groups studied. Moreover, primary NE was found to be more frequent than secondary NE. The prevalence of primary NE was 82%, making the prevalence of secondary NE to be 18%.
Analysis of the frequencies of children with a family history of bedwetting and social-related factors of children who are patients of primary healthcare in Bahrain are shown in Table 3.
Results regarding associations between NE and age, gender, parental employment and education, number of siblings, birth order, family history, parental divorce or conflicts, decease of a parent, constipation, and fluid intake before sleep are shown in Tables 4, 5, and 6.
Table 3: Frequency of family- and social-related factors in children who were patients of primary healthcare
in Bahrain
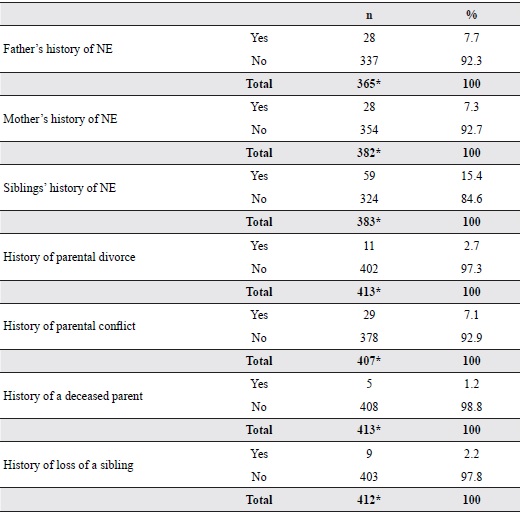
*The difference between the sample size (n = 438) and the total sample size mentioned in the table is due
to missing data.
Table 4: The association of nocturnal enuresis with the demographic characteristics of children and their
parents who attended primary healthcare
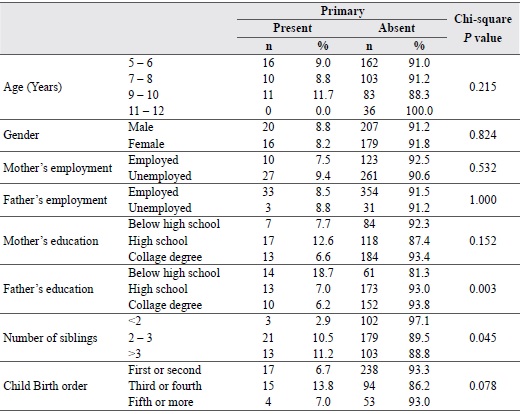
Table 5: The association of nocturnal enuresis with the family related and social characteristics of children
and their parents who attended primary healthcare
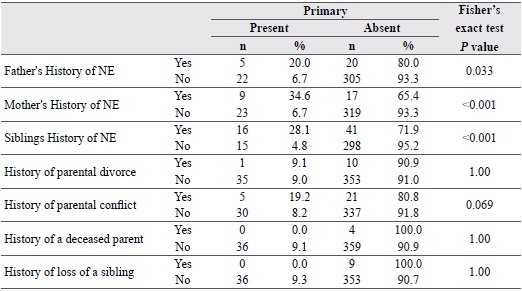
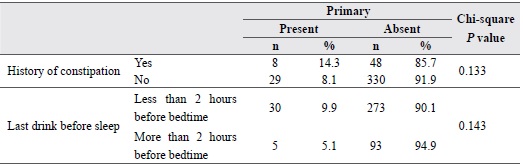
Table 6: The association of nocturnal enuresis with health and behavioral conditions of children and their
parents who are attending primary health care
An overall prevalence of NE of 11.1% is close to the prevalence found in other studies.3, 12 Primary NE, found in 8.7 % of the total population, accounts for 82 % of children with NE. This study found that there was no difference in the frequency of NE as the age increased. In contrast, a study done in Yemen showed that NE significantly decreased with age, from 31.5 % at 6–8 years to 8.7 % at 15+ years (P < 0.05).4 This trend (decrease in prevalence with increase in age) was also found in other studies.3, 5,6, 8, 12
In this study, gender did not have a significant effect on the prevalence of NE. Similar results were found in other studies.3, 4, 6, 12 However, male predominance in NE patients was detected in studies in India and Turkey.1, 16 A study8 conducted in the Kingdom of Saudi Arabia among primary school children, indicated that the frequency of enuresis was significantly higher among girls than boys (P < 0.001). Therefore, no consistent relationship between gender and NE has been discovered.
When the data was analyzed, mother’s (P = 0.532) and father’s (P = 1.000) employment was found to have no significant relationship with NE. This is in contrast to Yousef et al.’s study4, that showed the father’s working status having a significant association with the occurrence of enuresis. On the other hand, studies6, 12 performed in the Menofia Governorate (Egypt) and the northwest of Turkeyfound that an employed mother would have less children diagnosed with NE compared to a housewife (OR 0.27, CI [0.11; 0.68]; P < 0.05).
The relationship between the education level of the father and NE in his children was significant. A higher paternal education level led to a decrease in the prevalence of NE in his children. A mother’s education level, on the other hand, was not found to be related to the risk of NE in her children. This finding was thought to be due to socioeconomic status increasing with the increased education level of the father since he is considered responsible for the family’s financial support in the Bahraini culture. A study in Egypt supported the finding of this study, showing that fathers (P = 0.05) and mothers (P = 0.001) with higher education levels have less children diagnosed with NE.12 In contradiction, a study3, completed in Turkey, reported that there
was no association between enuresis and parental education (P > 0.05).
The number of siblings a child has, was found to be related to NE in this study (P = 0.045). A similar result was found in a study16 in Turkey (P = 0.003). In this study, a family factor found not to be significantly related to NE was birth order. Similarly, a study4 done in Aden Governorate (Yemen) revealed that birth order had no relationship with NE. In contrast, a study12 conducted in the Menofia Governorate (Egypt) presented a significant result in terms of the relationship between birth order and NE (P < 0.001).
In this study, an important risk factor found to be associated with NE was family history. This association is consistent with a study in school children in the Aden Governorate (Yemen).4 Family history was seen to have a significant association with the occurrence of enuresis in the studied students, accounting for 37.2 %, compared to 9% among those with negative family history (P < 0.005). Moreover, a study16 in Turkey showed that there was a significant relationship between NE and a sibling having a positive history of NE. This supports the findings of this study.
In this analysis, the separation or divorce of parents was not found to have an association with NE (P = 1.00). A study9 conducted in Taiwan was in disagreement, showing that separated or divorced parents are important factors associated with enuresis. The reason behind this discrepancy may be that the number of patients in this study, who had divorced parents, was small (did not exceed 3 %). Therefore, the significance of the variable’s relationship with NE might have been difficult to determine. The relationship between NE and a deceased parent was not significant (P = 1.00). Similarly, a study16 executed in Turkey, which reported associations of each parent’s death, found that there was no significant relationship between the death of either a mother or father and NE.
A study5 was conducted in Benha, Egypt showing that constipation was found in 66.7 % primary enuretic
children and 33.3% secondary enuretic children (P = 0.05). Moreover, a study14 was conducted in Turkey showing that constipation was found in 7.06 % enuretic patients, a statistically significant percentage (P = 0.0001). Similarly, a study17 was carried out in Malatya, Turkey in school children aged 5–9 years showing a significant relationship between NE and constipation. Among constipated patients, the frequency of enuresis was 21.6 % compared to 7.8 % in nonconstipated children (P < 0.05). This study found an insignificant relationship between NE and constipation (P = 0.133). In this study, an insignificant relationship was found between NE and the last drink before sleep (P = 0.143). This result is similar to that found in a study9 conducted in Taiwan.
The overall prevalence of NE in Bahrain is 11.1 %, and the overall prevalence of primary NE is 8.7 %. The prevalence of primary NE, in NE patients, is 82 %, and the prevalence of secondary NE, in NE patients, is 18%. These results are similar to other studies. There is a significant relationship between primary NE and the level of education of the father, number of siblings, and family history of NE.
We acknowledge the supervision of Dr. Adel Al Sayyad, the revision and feedback from all the committee members, and the assistance and cooperation of all health center staff, who helped us in the data collection process. We also appreciate the time and effort of Mr. Hasan Al Basri from the statistics department of Ministry of Health.