
Total Articles: 43
Today's Visitors: 40

Journal of the Bahrain Medical Society
Year 2018, Volume 30, Issue 3, Pages 20-24
https://doi.org/10.26715/jbms.3_22122018Ahmed Abduljalil Al Rashed1*, Qasim M.A. Isa2
1Intern, Salmaniya Medical Complex, Manama, Kingdom of Bahrain.
2Senior Urology Resident, Salmaniya Medical Complex, Manama, Kingdom of Bahrain.
*Corresponding author:
Ahmed Abduljalil Al Rashed, Intern, Salmaniya Medical Complex, Manama, Kingdom of Bahrain; Tel: (+973) 34546959, Email: aj_alrashid@hotmail.com
Received date: September 18, 2018; Accepted date: December 22, 2018; Published date: December 31, 2018

Background and objectives: Benign prostatic hyperplasia (BPH) and overweight (BMI: > 25–30 kg/m2) are both highly prevalent amongst Bahraini males. The aim of this study is to evaluate the association between BPH and overweight.
Methods: The study included 141 male patients who visited the Urology outpatient clinics between 1st April 2018 and 31st May 2018. Body mass index (BMI) was calculated and diagnosis of prostate enlargement was recorded along with prostate volume (ml) and prostate specific antigen (PSA). The collected data were analyzed using SPSS 23. Pearson correlation coefficient “r” and regression analysis were performed for prostate volume and PSA in relation to BMI. P < 0.05 was considered statistically significant.
Results: Among 141 male patients, 67 (47.5%) were overweight and had prostate enlargement, 50 (35.4%) were overweight with normal prostate, 10 (7.1%) were normal weight with prostate enlargement, and 14 (10.0%) had normal weight with normal prostate. The odds ratio was calculated as 1.876. This signifies that an overweight male is at 1.876 times higher risk of developing prostate enlargement compared to a male with normal weight. Overweight had a statistically significant positive linear correlation with incremental increases in prostate volume (r = 0.4; B = 0.85; P = 0.012).
Conclusion: There is evidence to support the hypothesis that overweight BMI is associated with a higher risk of development of prostate enlargement. The higher the BMI, the larger the prostatevolume; however, the same association was not observed with PSA.
Keywords: Benign prostatic hyperplasia, body mass index, overweight, prostate specific antigen, prostate volume
According to the World Health Organization (WHO), overweight (Body mass index (BMI): > 25–30 kg/m2) and obesity (BMI: > 30 kg/m2) are defined as“an abnormal or excessive fat accumulation that may impair health”.1 Overweight is regarded as a major risk factor in the development of multiple diseases and comorbidities.2 Diabetes mellitus, hypertension, and ischemic heart disease are some of the widespread noncommunicable diseases that have been strongly associated with a long-standing history of overweight.2 However, overweight has been projected as the most modifiable risk factor among preventable causes of death.2 BMI is calculated through measurements of the individual’sweight and height and commonly used to classify overweight and obesity in adults.
Similarly, benign prostatic hyperplasia (BPH) isa prevalent disease, mostly affecting elderly men. It is defined as “the proliferation of epithelial and smooth muscle cells within the transition zone of the prostate”.3 It is considered as a disease of aging due to the increasing incidence of developing BPH with age. The prevalence of BPH reaches 80% in men over 80 years of age.4
It’s been hypothesized that the development of BPH is related to an increase in the levels of estrogen to androgen ratio, which is associated with increase in weight, particularly abdominal obesity.5Furthermore, another possible relation would be that overweight leads to chronic insulin resistance, and hence, chronic elevation in blood insulin levels.The elevated levels of blood insulin concurrently lead to increase in the synthesis of insulin-like growth factor-1 (IGF-1) and availability in the bloodstream as well. Both, insulin and IGF-1, impact the development of hormonally driven tumors, such asprostate cancer and may stimulate BPH.6
According to the WHO, in 2007, the Kingdom of Bahrain had an extremely high incidence of overweight population, wherein 33% of the population aged > 20 years 7 This was significantly higher than the worldwide incidence of overweight, which was 12%.7
The aim of this research is to determine the association between overweight and BPH. Concurrently, this study aims to determine correlation between overweight and higher prostate volume (ml) and a higher prostate specific antigen (PSA).
The present retrospective study was conducted in Salmaniya Medical Complex (SMC), Kingdom of Bahrain. It was approved by the Secondary Health Care Research Subcommittee (SHCRC), SMC, Ministry of Health, Kingdom of Bahrain.
The study included male patients who visited the department of Urology in SMC for any reason between 1st April 2018 and 31st May 2018. Simple random sampling was employed to select the patients. A sample size of 100 patients was considered to be sufficient in order to be able to calculate an accurate Pearson correlation coefficient. This was based on both the prevalence rate of BPH—it increases from 8% in men aged 31–40 years to 40–50% in menaged 51–60 years and to over 80% in men older than 80 years4—as well as the patient pool who attended outpatient clinics at SMC.
The exclusion criteria for this study’s sample werefemale patients, bedridden patients (unable to stand for height and weight measurement), patients undert he age of 30, and patients with prostate cancer diagnosis. The total sample size in this study was 141 patients after the exclusion of 53 patients from data collection according to our exclusion criteria.
All data were obtained through the National Health Information System (I-SEHA) of Bahrain’s Ministry of Health at SMC. All the data were extracted by a single reviewer. The data obtained included patients age, height, and weight, which were measured using the outpatient clinic scales, and were used to calculate the BMI. Any previous diagnosis of prostate enlargement that is documented in the patient file on I-SEHA system was recorded along with prostate volume through prostate ultrasound and PSA level, if they were done for the patient.
Classification of BMI of patients was determinedby referring to the WHO International BMI Classification.1 In order to evaluate the influence of overweight BMI on the presence or absence of the disease (enlarged Prostate), the odds ratio (OR) was calculated. In addition, it will aid in determining the odds of developing prostate enlargement in overweight males.
The data were analyzed using SPSS 23. Pearson correlation coefficient “r” and regression analysis were calculated to evaluate positive or negative linear correlation between overweight and high prostate volume and PSA.
All the patients were males of Bahrain nationality.The mean age of the patients was 60.9 years. The majority of the sample was overweight, comprising 117 patients (82.9%) of the entire sample with an average BMI of 30.7 kg/m2. A total of 77 (54.6%) patients were diagnosed of prostatic enlargement.
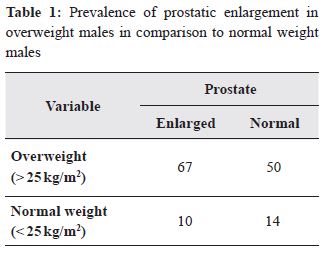
We found that out of the 141 patients, 67 patients (47.5%) were overweight and had prostate enlargement, 50 patients (35.4%) were overweight with normal prostate, 10 patients (7.1%) were normal weight with prostate enlargement and 14 patients (10.0%) were normal weight with normal prostate.
Incorporating Table 1, OR was calculated (OR = 1.876). This signifies that an overweight male has 1.876 times higher odds of developing prostate enlargement compared to a normal weight male.
The data shown in Table 2 demonstrates that the patients were mostly in the fifth and sixth decades of life. Since SMC is a tertiary hospital covering all of Bahrain, the data in Table 2 demonstrates that older males in their late fifties to early sixties compromise a significant number of the Urology OPD clinic visits in Bahrain. '
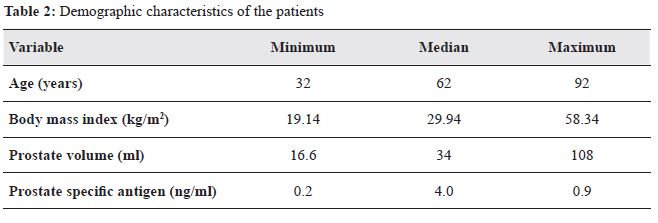
Furthermore, a significantly higher number of overweight males were present in this random sample, comprising 117 (82.9%) of the total sample. This finding coupled with the average and median BMI, in Table 2, reflects a high prevalence of overweight and obesity in males aged > 30 years in Bahrain. The median prostate volume was 34 ml, which is higher than the normal prostate volume (25ml).8 This finding reflects that the median prostate volume amongst our sample is high.
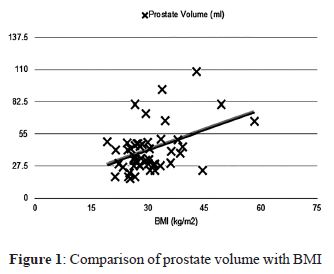
Figure 1 compares the prostate volume with BMI and demonstrates a positive linear relationship between the two variables, which aids in the conclusion that the higher the BMI, the larger the prostate volume. Moreover, overweight patients had a statistically significant positive linear correlation with incremental increases in prostate volume (r = 0.4;B = 0.85; P = 0.012; Figure 1). Further, overweight patients had a statistically nonsignificant negative linear correlation with influential decrease in PSA(r = -0.08; B = -0.01; P = 0.515).
Obesity and BPH are globally prevalent conditions and multiple comorbidities are associated with overweight individuals. The fact that prostatic enlargement can be associated with increase in weight adds further reason for the general male population to pursue an active, healthier lifestyle and aim to avoid obesity.
In this study, it specifies that overweight significantly increases the odds of developingprostatic enlargement compared to individuals with normal weight. Therefore, we interpret that there is an association between higher BMI and having a higher prostate volume. However, the same association was not observed in regard withP SA.
Similarly, a retrospective cohort study conducted in South Korea by Jung JH et al. revealed that increase in body weight and fat composition was significantly associated with the presence of higher prostate volumes.6
Dahle SE et al. studied body size and serum levels of insulin and leptin in relation to the risk of BPH. The study demonstrated that increase in abdominal obesity and serum insulin levels are associated with higher risk of BPH.9 These studies further correlate with the results obtained in this study and support evidence that higher serum insulin levels that are associated with an increase in body weight can impact prostate enlargement.
One limitation that was faced was that not all prostate ultrasounds were performed by a single radiologist doctor. Since ultrasound is an operator dependent investigation, slight variations in prostate volume measurements could be present. Moreover, measurements of patients’ weight and height were carried out by different nursing staff members, which might also affect the measurements leading to altered BMI calculation.
However, in this study, PSA levels of all the patients were measured at the same laboratory located in SMC and the same weight and height scales were used for all the patients, which adds to the accuracy of the measurements obtained.
According to our findings, we conclude that there is evidence to support that the overweight patients have a significantly higher risk of developing prostate enlargement and higher prostate volumes. However,the same association was not observed with PSA. Further, research should be conducted in order to better understand the impact of different stages ofobesity on progression of prostatic hyperplasia. In addition, further evaluation is required to assess influence of presence of other comorbidities on development and progression of BPH.
The authors of the study have no conflict of interest to declare.
Special thanks to Dr Said Taan EL Hajjar, Associate Professor, Acting Dean, Ahlia University, Kingdom of Bahrain, for his help with the statistical analysis.