

Journal of the Bahrain Medical Society
Year 2018, Volume 30, Issue 1, Pages 9-13
https://doi.org/10.26715/jbms.1_10122017Khawla Saad Ahmed Mandoos1*, Elham Atalla1, Amaal Al Thawadi1, Hana Ahmed Alfayez2
1Primary Care Directorate, Ministry of Health PO Box 42, Kingdom of Bahrain.
2Ministry of Health PO Box 42, Kingdom of Bahrain.
*Corresponding author:
Khawla Saad Ahmed Mandoos, Primary Care Directorate, Ministry of Health, PO Box 42, Kingdom of Bahrain; Tel: (+973) 32-249977, Email: KSaad1@health.gov.bh
Received date: January 03, 2017; Accepted date: December 10, 2017; Published date: March 20, 2018

Background and objectives: Sexual dysfunction is one of the most common but considerably less explored female sexual problems in the Arabian world. This study provides insights into the prevalence of this problem in Bahraini women. To explore the prevalence and various aspects of the female sexual dysfunctions (FSD) in Bahraini women.
Methods: This is a cross-sectional study which involved the collection of FSD data. The subjects were selected, in equal numbers, from four health centers in the Kingdom of Bahrain. Female Sexual Function Index (FSFI) was used in this study.
Results: This study established that FSD is highly prevalent in Bahraini women (55.8%) and is associated with various features and characteristics. Many demographic and health risk factors of FSD were identified, including wife’s and husband’s age, female’s education and employment status, duration of the marriage and the number of children, as well as the presence of chronic illnesses such as diabetes mellitus and hypertension. In addition, it has been demonstrated that the awareness of the availability of sexual healthcare services was poor amongst women attending the healthcare centers, with 73% of women indicating they had no prior knowledge of such a facility.
Conclusion: Prevalence of FSD in Bahrain is high, and more attention should be directed toward this problem. Most women, however, seem to be unconcerned with their FSDs. Most subjects in this study were unaware of the existence of sexual healthcare facilities. A planned follow-up study is warranted to further understanding of FSD in Bahraini women.
Keywords: Female sexual dysfunction, Female Sexual Function Index
Sexual dysfunctions are a group of related disorders which are typically characterized by a disturbance in a person’s ability to respond sexually or to experience sexual pleasure.1 WHO defines female sexual dysfunction as various ways in which a woman is unable to participate in a sexual relationship as she would wish.2 These disorders have a prevalence of approximately 40% in men, where male erectile dysfunction is the most common type of sexual dysfunction3, and 19-50% in women.4 Sexual disorders have a big effect on interpersonal relations, personal satisfaction and overall quality of life. This study investigates the prevalence of female sexual dysfunction in Bahraini women and the variables that can influence their occurrence to improve the quality of care and the service offered to female patients with sexual dysfunctions and other difficulties.
Sexuality is an integral part of human life; reproduction and general wellbeing.5 Female sexual dysfunction (FSD) is defined as a collective, multifactorial and progressive problem relating to sexual health and wellbeing and can cause pain during the sexual encounter.6 This problem is difficult to diagnose and treat because of the intricacy of the female sexual response. There are two prominent views on how the female sexual response cycle works. One is proposed by Masters and Johnson in 1966 who assumed that there is no difference between male and female sex response cycle. This is called the linear model and entails that there are four stages of the sexual response cycle beginning with excitement/arousal and proceeding to plateau, orgasm, and resolution.7
In 1998, the Sexual Function Health Council of the American Foundation of Urologic Disease revised pre-existing definitions and classifications of female sexual dysfunction (FSD).8 Medical risk factors, etiology, and psychological aspects were classified into four categories of FSD: 1) desire, 2) arousal, 3) orgasmic disorders, and 4) sexual pain disorders.
General objectives of this study were 1) To obtain data on the prevalence of FSD in women in Bahrain, 2) To identify factors closely associated with FSD in women in Bahrain and 3) To catalog data that could be useful for the future directions of healthcare policymaking in Bahrain.
Data were collected from 201 married women who attended primary health care centers by using the Female Sexual Function Index (FSFI) questionnaire (Appendix 1). The Arabic translation of the FSFI in this study was adapted from a previously published study.9
The subjects were selected, in equal numbers, from 4 health centers in one region of the Kingdom of Bahrain. The main inclusion criteria included i) gender, ii) marital status, iii) age, iv) ability to give consent, v) ability to read Arabic and vi) whether the husband was alive. All randomly selected women were invited to attend a face-to-face interview with one of our female authors. Privacy and confidentiality were assured. The structured interviews were based on the19-items. For individual domain scores, scores of the individual items that comprise the domain were multiplied by the domain factors, where higher scores indicate less dysfunction.
All the six domains score were added to obtain a final full score. The confidentiality of information regarding the research was provided in written form and consent was given by completing the questionnaire.
Demographic data including age, occupation and employment status was also recorded. The presence of hypertension, dyslipidemia, diabetes, and coronary artery disease was documented depending on the women’s history.
Analysis of the data was performed using the computer program Statistical Package for Social Studies (SPSS) version 11.5. A series of chi-square tests were used to identify which risk factors (both socio-demographic and health) are significantly associated with FSD.
Our preliminary data is based on 201 women aged between 18 and 64, more than 50% of whom (Frequency = 107) were aged between 25 and 54 at the time of data collection. More than 80% of the women (Frequency = 179) were educated to the at least secondary school level, and more than 50% (Frequency = 109) were employed. Still, our initial studies suggest that most of the women were unaware of the existence of any sexual healthcare services, with 73% of women indicating that they had no prior knowledge of such facilities.
Descriptive statistics for each of the domain scores as per illustrated in Table No.1 as well as for the overall score are presented in Table 2.
Following a previous study conducted in Egypt, the overall score of 28.1 (78% of the maximum that equals 36 points) was taken as the cut-off point for the FSFI to distinguish between the women with FSD and the women with normal function10.
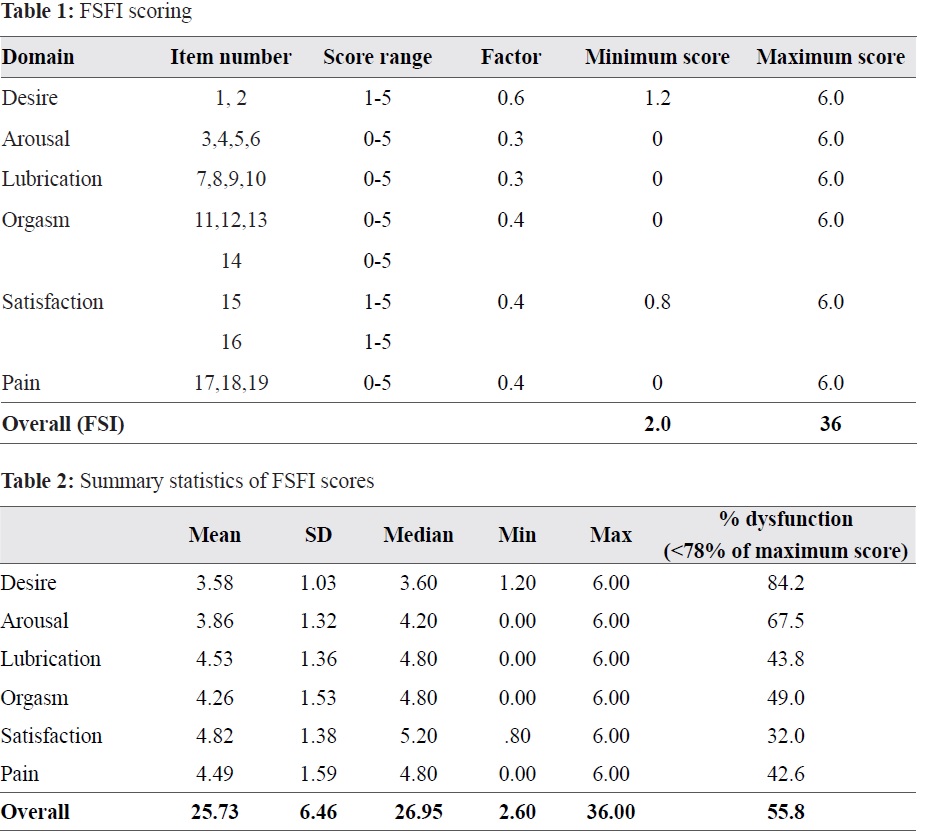
According to this criterion, 55.8% of surveyed women had FSD, which indicates a high prevalence of FSD in Bahraini women. Similarly, females whose domain score was lower than 4.7 (i.e., 78% of the maximum domain score of 6) were considered to have problems with the corresponding sexual function domain. According to this criterion, 84.2% of the respondents suffered from desire problems, while only 32% - from satisfaction problems (Table 2).
It has been found that 32.7% of respondents reported lack of desire. In addition, it was demonstrated that 48.2% had difficulty in achieving and 34.8% in maintaining the sufficient level of lubrication during sexual intercourse.
The survey found that only a 10% (Frequency =20) of women had any complaint about their ability to reach orgasm or were dissatisfied with their sexual intercourse encounters. Pain during or after intercourse was found among 35.4% (Frequency =71) of the study subjects.
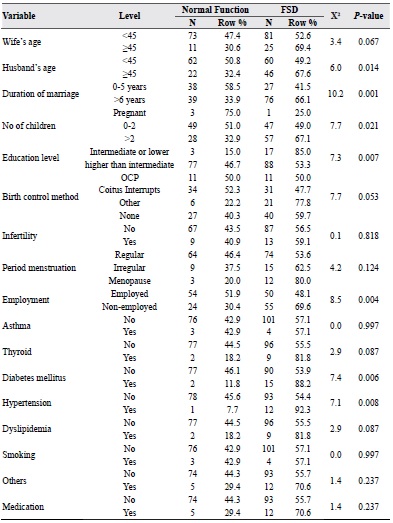
A series of chi-square tests were used to identify which risk factors (both socio-demographic and health) are significantly associated with FSD. It appears that the following groups of women have significantly higher probability of suffering from FSD: women whose husband’s age is more than 44 (68% have FSD); those who have been married for more than 5 years (66%); women with more than two children (67%); females with an intermediate, primary or no education (85%); and non-employed women (70%). In addition, diabetes mellitus and hypertension are strong predictors of FSD: in our sample, women suffering from these health problems had FSD in 88% and 92% of cases, respectively. It is worth mentioning that wife’s age, birth control method, thyroid, and dyslipidemia were found to be significant risk factors at 10% level (Table 3).
Table 3: Risk factors associated with female sexual dysfunctions
In this preliminary study, we have shown that Bahraini women are approachable to carry out a survey on sexuality with a response score of nearly 100%. Our survey, though small, has highlighted some crucial issues related to sexuality in Bahraini women. While many of the women expressed varied levels of satisfaction, there were cases of complete dissatisfaction with sexual life. There were also cases where women complained of difficulties in achieving or maintaining a sufficient lubrication and experiencing pain during and or following penetration. These factors could be indicative of the presence of FSD in some forms. Further investigation would reveal the cause and effect of these complaints with FSD in Bahraini women.
This study has the limitation of including only married women which might lead to exclusion of more cases such as single, widowed, and divorced females. In any future study, this should be noted, and the efforts should be directed at recruiting the women from the categories underrepresented in this study.
Similar to the findings of Egyptian study, we have found that a major proportion of women in Bahrain have FSDs manifested in at least one of many forms. While employment and educational status were not identified as major contributory factors by our study, it is possible that the family relationship and the age of women are significant contributory factors pre-disposing Bahraini women to sexual dysfunction.8, 10
While a case can be made that since the data was collected from clinics and healthcare centres it might result in a higher percentage of cases of FSD and not represent the community level prevalence of FSD, it is important to base our studies on such cases to make faster progress in forwarding this field of study in Bahrain.
This study found that there is clear case of occurrence of FSD in Bahraini women. It has been revealed that certain socio-demographic groups are at a higher risk of FSD. In addition, women with diabetes mellitus and hypertension have a significantly higher probability of FSD.